The progression of severity of disease can be underestimated
Download the following echocardiographic guide for a review of common challenges and special considerations specific to severe aortic stenosis.
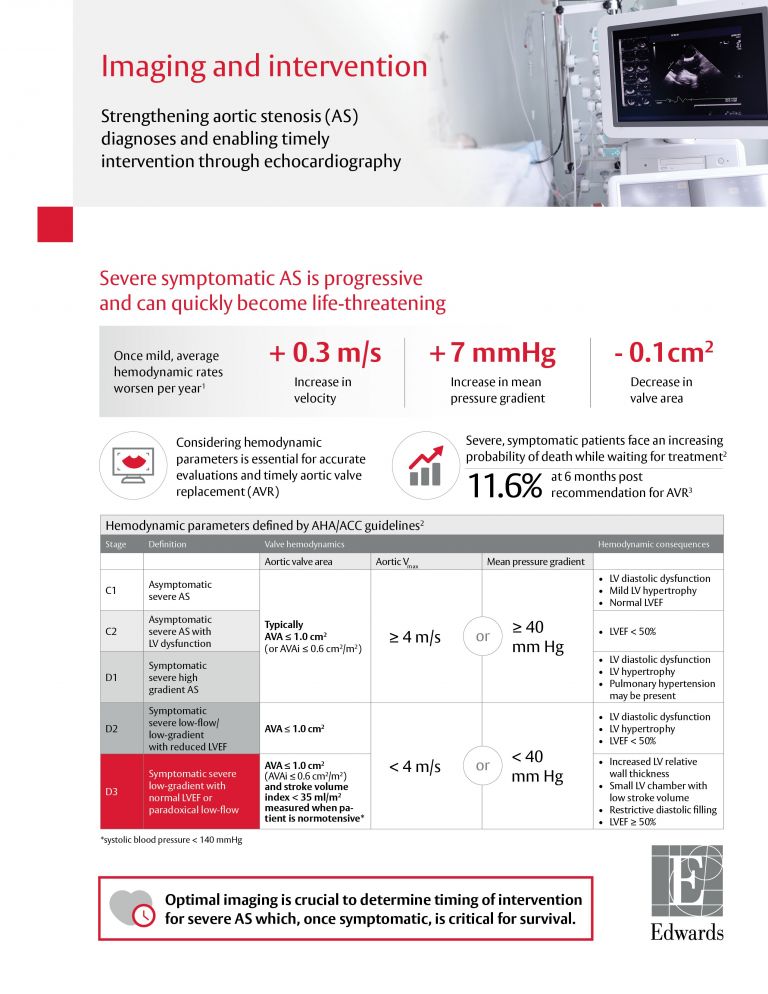
The detection of severe aortic stenosis (AS) may be missed in up to 50% of severe AS cases until post-mortem.1 Symptom onset may be subtle and overlooked by the patient, so relying on an echocardiogram is critical to determine disease progression. The ACC Guideline recommends a comprehensive transthoracic echocardiogram (TTE) be performed for known or suspected valve disease. And regular follow-up with TTE should be performed at least yearly to evaluate a patient’s symptoms and disease progression once advanced to severe AS.
Considering hemodynamic parameters is essential for accurate evaluations and timely aortic valve replacement.
Hemodynamic parameters for symptomatic severe AS defined by ACC/AHA Guideline1
Select a stage to see the related data:
Definition
Symptomatic severe high gradient AS
Valve hemodynamics
Hemodynamic consequences
Definition
Symptomatic severe AS
Valve hemodynamics
Hemodynamic consequences
Definition
Symptomatic severe
Valve hemodynamics
*Systolic blood pressure < 140 mm Hg.
Hemodynamic consequences

Avoid the underestimation of LVOT area and thus underestimation of flow rate2

Patients with lower than expected gradients despite preserved LVEF can lead to an underestimation of severity, which may delay aortic valve replacement6

Use baseline and low-dose dobutamine stress echocardiography to differentiate between true and pseudo severe AS in those with reduced LVEF4
References: 1. Das P, et al. The patient with a systolic murmur: severe aortic stenosis may be missed during cardiovascular examination. Q J MedJ 2000;93:685-688. 2. Baumgartner, H. (2017). Recommendations on the Echocardiographic Assessment of Aortic Valve Stenosis: A Focused Update from the European Association of Cardiovascular Imaging and American Society of Echocardiography. JASE, 30:372-92. 3. Malaisrie, C. (2014). Mortality While Waiting for Aortic Valve Replacement. Ann Thorac Surg 98:1564-71. 4. Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(23):2440-92. 5. Clavel MA, Magne J, Pibarot P. Low gradient aortic stenosis. Eur Heart J. 2016; 37(34): 2645–2657. 6. Dumesnil, J. G. (2009). Paradoxical low flow and/or low gradient severe aortic stenosis despite preserved left ventricular ejection fraction. EHJ, 31(3), 281–289.