Clinical data on surgical valves with RESILIA tissue up to 7-year follow-up have been published, with additional follow-up to 10-years in progress.8
References:
1. Tarantini G, Fovino LN, Le Prince P, et al. Coronary access and percutaneous coronary intervention up to 3 years after transcatheter aortic valve implantation with a balloon-expandable valve. Circ Cardiovasc Interv. 2020;13(7):e008972.
2. Tarantini G, et al. Redo-Transcatheter aortic valve implantation using the SAPIEN 3/Ultra transcatheter heart valves – Expert Consensus on Procedural Planning Techniques, The American Journal of Cardiology, 2023
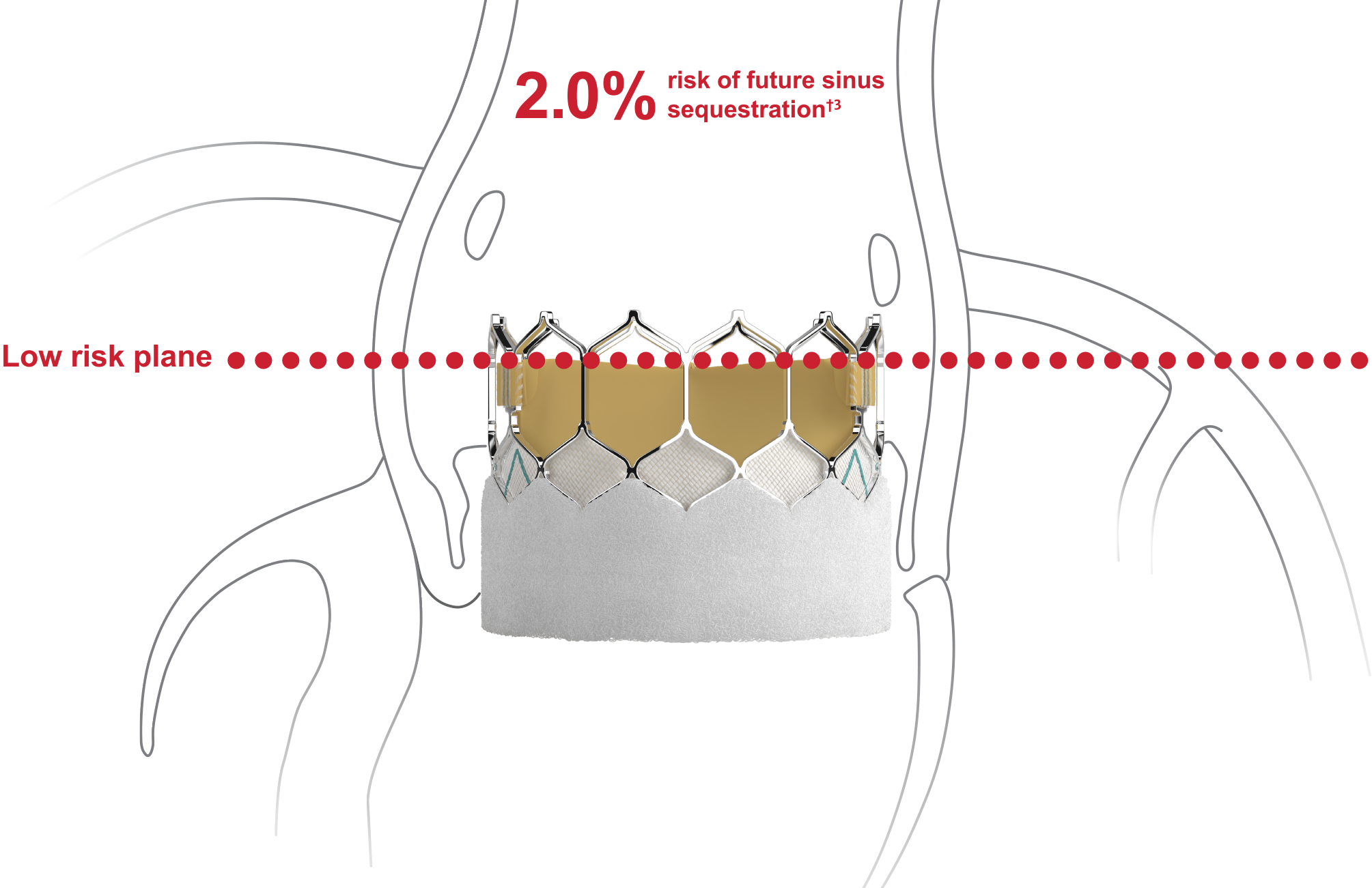
3. Ochiai T, Oakley L, Sekhon N, et al. Risk of coronary obstruction due to sinus sequestration in redo transcatheter aortic valve replacement. JACC Cardiovasc Interv. 2020;13(22):2617-2627. doi:10.1016/j.jcin.2020.09.022.
4. De Backer O, Landes U, Fuchs A, et al. Coronary Access After TAVR-in-TAVR as Evaluated by Multidetector Computed Tomography. JACC Cardiovasc Interv. 2020;13(21):2528-2538.
5. Edwards Lifesciences SAPIEN 3/Ultra valve Instructions for Use.
6. Makkar RR, et al. Outcomes of repeat transcatheter aortic valve replacement with balloon-expandable valves: a registry study. Lancet. 2023 Aug 31:S0140-6736(23)01636-7.
7. Leon MB, Mack MJ, Pibarot P et al. Transcatheter or Surgical Aortic-Valve Replacement in Low-Risk Patients at 7 Years. N Engl J Med. 2025
8. Beaver T, Bavaria JE, Griffth B, et al. Seven-year outcomes following aortic valve replacement with a novel tissue bioprosthesis. J Thorac Cardiovasc Surg. 2024;168(3):781-791. doi:10.1016/j.jtcvs.2023.09.047
9. Makkar R. Ten-year outcomes of the PARTNER 2 intermediate-risk studies: a propensity-matched analysis of P2S3i TAVR and P2A surgery. Presented at: TCT 2025; October 27, 2025; San Francisco, CA